














































































In the arsenic of modern dermatocosmetology today, there is a fairly wide range of methods for correcting various aesthetic irregularities in the skin - chemical peels, mechanical dermabrasion, laser surface treatment, microdermabrasion, contour plastics. .
This trend is particularly typical of hardware methods, primarily for laser medicine. The use of lasers, first in dermatology and then in cosmetology, has an impressive period. Even since the appearance of one of the newest laser treatment methods - selective photothermolysis - it has been more than 25 years. The pioneers in this field, the Americans RR Anderson and JA Parrish, predetermined the fate of fractionated lasers in the field of medicine, making them indispensable in the treatment of such an aesthetic skin imperfections as capillary hemangiomas. Port wine stains, hypertrichosis, tattoos, rosacea, pigmentation disorders, photography, wrinkles, etc.
Modern skin rejuvenation techniques
We live in a time when more people are living to old age than ever before. And given that many of them continue to lead an active life, one of the most important problems in aesthetic medicine is the fight against aging skin.
Plastic surgery is able to rejuvenate the shape of the face by removing excess skin. At the same time, however, the skin still remains after time (age-related aging) or external factors (photography). It is also important that most patients want it to look younger without surgery.
What method should be used in this case to affect the skin, and what should be done in it for its real rejuvenation?
All methods that can be used to improve the appearance of the skin are united according to one principle - they use a traumatic effect on the skin and cause fibrosis, which further leads to its tension and compression.
Currently, dermatocosmetology uses three main types of skin rebuilding effects, including:
- chemical stimulation - chemical peels with acids (trichloroacetic acid, glycolic, etc. );
- mechanical stimulation - mechanical dermabrasion, microdermabrasion, mesotherapy, fillers, subcision with needles;
- thermal stimulation - laser ablation, thermolift using lasers and broadband light sources, radio frequency boost, fractional methods.
Chemical stimulation
Historically, acidic exfoliation (peeling) was the first method of skin rejuvenation. The principle of peeling is partial (as with superficial peeling) or almost complete (as with medium and deep peeling) destruction of the epidermis, which damages fibroblasts and dermis structures. This damage activates an inflammatory reaction (the more powerful, the greater the volume of destruction itself), leading to further production of collagen in the skin.
To achieve the desired result, peeling must sacrifice the epidermis. Experiments with burns have misled many, allegedly "proving" that the epidermis is a self-renewing organ that quickly recovers from the damaged area. In this regard, peels became for a while more and more aggressive towards the epidermis (e. g. , deep phenolic peeling), until the accumulated problems eventually made specialists realize the evil by the method that eventually leads to thinning of the skin.
Proponents of deep peeling ignored the new issues. Their essence was that due to the destruction of papillae in the dermis and the weakening of nutrition, the epidermis becomes thinner and the number of cells in the prickly layer is significantly reduced compared to what was before the peeling. A decrease in the barrier function of the stratum corneum leads to a decrease in skin hydration. (Therefore, after deep peeling for a long time, almost all patients experience severe dryness of the skin) At the same time, the introduction of practice-light peels (using trichloroacetic acid and fruit acids) did not live up to their hopes of tightening the skin effectively.
Mechanical stimulation
Of the methods of mechanical stimulation of involuntary changes in the skin, dermabrasion using rotating devices (at a speed of v; rotation of cutters up to 100, 000 rpm) deserves special attention. Currently used modern Schumann-Schreus devices (Germany)The method can only be used in a surgical hospital, as the procedure requires anesthesia, postoperative treatment of the wound surface, a special toilet for eyes and mouth, as well as equipment feeding patients (due to the fact that the pronounced postoperative edema that occurs2-3 days after the procedure, making it difficult to open eyes and mouth).
The method is very effective, but unfortunately with mechanical dermabrasion there is a high risk of complications such as:
- persistent postoperative hyperemia;
- occurrence of depigmentation areas due to destruction of melanocytes when the insert penetrates the basement membrane;
- infection of the wound surface;
- scarring (if the knife is too deeply immersed in the skin)
All of the above have determined the limited application of this method in clinical practice.
Thermal stimulation
Ablative conversion
Since the late 1980s, a laser has been used to rejuvenate the skin by layer-by-layer ablation [4]. Careful, low-traumatic removal of the skin surface layer by means of a carbon dioxide laser stimulates the synthesis of its own collagen therein, the size of which increases several times after the procedure. Then it is gradually reorganized.
The most effective was the use of a CO2 laser when exposed to a deep thermal effect on all layers of the dermis, externally manifested by the effect of skin tightening. The method is called "laser dermabrasion" or "laser resurfacing", and in terms of effectiveness, it could not be opposed to any other method of skin rejuvenation that existed at the time (Fig. 1).
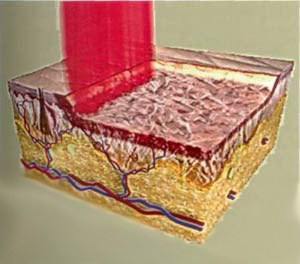
FIG. 1. Scheme with traditional laser skin surface treatment (laser dermabrasion)
However, theCO2 laser also causes a large number of complications. Further studies have shown that such a profound effect on the dermis stimulates the formation of fibrous tissue to a greater extent than contributes to the synthesis of a new, normal-oriented collagen [5]. Developed fibrosis can make the skin look unnaturally pale. Collagen synthesized after treatment is resorbed after a few years, as is all collagen formed at the site of the scar. As a result of thinning epidermis caused by atrophy in the papillary layer of the dermis, fine wrinkles begin to appear on the skin. Due to the weakening of the barrier function of the stratum corneum, the hydration level of the skin decreases and it looks atrophic.
Erbium-aluminum-yttrium grenade-erbium-lasers appeared somewhat later. Such advantages of an erbium laser as a lower thermal penetration depth (erbium lasers penetrate to a depth of 30 microns, CO2 lasers - up to 150 microns) and (as a result) the lower risk of burns and tissue carbonation as well as the relative cheapness (compared tocarbon dioxide lasers), attracted the attention of many specialists around the world.
As the experience of working with these two types of installations is gathered, the opinion has developed among specialists that CO2 lasers are more efficient [6]. Despite the negative effects of carbon dioxide laser abrasion described above, this method remains indispensable for the correction of acne scars. In addition, it can be considered as an alternative to surgical skin tightening - of all the methods for its remodeling, only exposure to a CO2 laser can actually cause a marked collagen contraction with visible clinical lifting effect.
The problem with all the methods described above is that they often "sacrifice", that is, significant damage to the epidermis. To rejuvenate your skin and really look young, you need a perfect epidermis with natural papules of the dermis, good hydration, normal skin tone and elasticity. The epidermis is a very complex highly specialized organ, up to 200 micrometers thick, which is our only defense against the effects of negative environmental factors. Therefore, no matter what we do to rejuvenate the skin, we need to make sure that its underlying normal architecture is never damaged.
This concept contributed to the emergence of non-ablative skin rejuvenation technology.
Non-ablative remodeling
The most common non-ablative skin rejuvenation devices are neodymium (Nd-YAG) and diode lasers as well as broadband light sources (IPL). The principle of their action - selective photothermolysis - consists in heating and destroying structures, containing a sufficient amount of melanin or oxyhemoglobin. In the skin, these are resp. Accumulations of melanocytes (lentigo, melasma) and microvessels (telangiectasia). The emitted wavelengths used in non-ablative lasers correspond to the maximum in the absorption spectra of oxyhemoglobin or melanin. The procedure of treatment with non-ablative lasers and IPL is quite safe, the rehabilitation period is minimal, but such treatment eliminates only pigmentary and vascular cosmetic defects. In this case, there is some thickening of the skin, but the effect obtained is short-lived.
Fractionated skin rejuvenation techniques
The constant search for new, highly effective and at the same time safe methods of skin rejuvenation has led to the emergence of a revolutionary technology - fractional delivery of laser radiation. The proposed skin rejuvenation method is specially designed to overcome some of the above difficulties. Unlike "conventional" ablative and non-ablative laser methods, which are designed to achieve uniform thermal damage to the skin at a certain depth, fractional methods allow to achieve its selective microscopic thermal damage in the form of several altered columns and leave unaffected areas aroundthese micro ulcers. Currently, the industry produces two types of fractional lasers: non-ablative and ablative.
The first uses an erbium-doped optical fiber that generates radiation at a wavelength of 1550 nm. The fractionated laser is formed in the skin thousands and tens of thousands of microdamages in the form of columns - microthermal treatment zones (MLZ) - with a diameter of 70-150mk depth up to 1359 mcm
As a result, approx. 15-35 skin on the treated area. The chromophore for the laser is water. Coagulation occurs mainly in the lower layers of the epidermis and dermis. The stratum corneum remains intact because it contains a relatively small amount of water, and this significantly reduces the risk of infection. Epidermal recovery is rapid due to the low lesion volume and the short migration distance of keratinocytes. The healing period is accompanied by moderate edema and hyperemia followed by desquamation occurring at 5-7. day. The patient practically does not lose social activity.
This technology - fractional photothermolysis (FF) - is a very effective method for non-ablative fractional skin rejuvenation. To achieve the desired effect, a course treatment is prescribed. Depending on the clinical situation, it is recommended to perform from 3 to 6 procedures with an interval of 4-6 weeks. As with any other method of renovating non-ablative skin, the final result can be seen 4-8 months after the procedure (cumulative effect).
In cases where a more aggressive effect on the skin is required - for the correction of scars, removal of deep wrinkles and excess skin, the method of fractional ablation (FA or fractional deep dermal ablation-FDDA) is used.
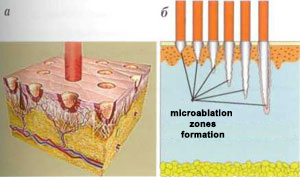
Fractional ablation method combines the benefits of a CO2 laser and the fragile principle of laser laser delivery. Unlike traditional CO2 lasers, which remove the entire skin surface layer by layer, the FA units form a huge number of microablating substance zones (MAL) up to 300 μm in diameter at an evaporation depth of 350 to 1800 μm (Fig. 2).
During this procedure, laser radiation penetrating the deep layers of the skin destroys the top layer of the epidermis. In terms of effectiveness, ablative fractional laser rejuvenation can be compared to plastic surgery. This is how deep the laser beam reappears.
FIG. 2. The principle of operation of the ablative fractional laser: formation of microablative zones - MAZ (a); dependence of the MAZ formation depth on the laser radiation power (b)
As with FF, 15 to 35% of the skin in the treated area is actually exposed (in some cases up to 70%). Recovery after the FA procedure is faster than after layer-by-layer ablation. This is due to the fact that significant part of the epidermis and stratum corneum remains intact. Skin bleeding is observed for some time immediately after the procedure, but soon stops (Fig. 3 a, b).
FIG. Step-by-step restoration of the skin after the fractionated ablation procedure: see immediately after treatment (a); every other day (b); after 5 days (c); 14 days (d) after a procedure

The patient's loss of social activity after the FA procedure lasts from 5 to 10 days.
To prevent scarring and manifestation of post-inflammatory pigmentation, it is necessary to carefully care for the skin. Decorative cosmetics can be used from 4-5 days. A prerequisite for a good result is the use of at least 3 months after the procedure for sunscreen cosmetics with a high degree of protection (SPF at least 50). The risk of post-inflammatory pigmentation occurs in 20% of patients and is generally higher in patients with skin IV-V phototypes. Such hyperpigmentation is transient and can last from 1 week to 3 months, which also depends on the depth of treatment and the area treated. For its prevention 1-2 weeks before the procedure and during a further 2 weeks after it, external agents based on hydroquinone (4%) and tretinoin (0. 1%) are prescribed. The main effects on the facial skin after the FA procedure are as follows: pronounced tightening and reduction of excess skin, smoothing of surface wrinkled skin as well as skin affected by acne scars, reduction of dyschromia, porosity.
This method was tested by the author and his colleagues to remove skin marks as well. As shown in clinical trials, the method has shown high efficacy in eliminating almost all types of stretch marks, both acquired during puberty and postpartum. It was noticed that the healing processes on the skin of the skin are different than on the skin of the face.
Skin remodeling mechanism using fractional lasers
Let's consider the mechanisms of skin remodeling when using fractional lasers.
After exposure to laser, aseptic inflammation develops in the area with the micro ulcers formed. The more aggressive the laser exposure, the more pronounced the inflammatory response, which actually stimulates the post-traumatic release growth factors and infiltration of damaged tissue by fibroblasts. The forthcoming reaction is automatically accompanied by an outbreak of cellular activity, which inevitably leads to the fact that fibroblasts begin to produce more collagen and elastin. The skin transformation process includes three classic phases of regeneration:
- Phase I change (tissue inflammation). Start immediately after injury;
- phase II - proliferation (tissue formation). Begins 3-5 days after injury and lasts approx. 8 weeks;
- phase III - tissue remodeling. Lasts from 8 weeks to 12 months.
It should be noted that all three phases of skin remodeling are observed both after fractional photothermolysis and after fractional abulation. However, in the first case, the harmful effect of the laser is moderately aggressive, resulting in a cascade of inflammatory change is never too wild.
A completely different image is seen after exposure to the fractionated ablation laser. The trauma caused by this laser bursts blood vessels and blood cells along with serum are released into the surrounding tissue. The full mechanism of skin regeneration - pha change begins - aseptic inflammation develops. Platelets released from damaged vessels play an important role in activating blood coagulation and releasing chemotoxic factors, which in turn attract other platelets, leukocytes and fibroblasts. Leukocytes, especially neutrophils, participate in the cleansing of damaged tissue and remove fragments of necrotic tissue, which are partially destroyed by phagocytitis, and partially reach the surface of the skin in the form of microscopic debris consisting of epidermal and dermal tissue substrates and melanin - microepidermal necroticwaste (MENO).
The proliferative phase begins in approx. 5 days. During this period, neutrophils are replaced by monocytes. Monocytes, keratinocytes and fibroblasts continue to affect growth factors and are at the same time under their inverse influence. keratinocyte stimulate the growth of the epidermis and the release of growth factors necessary to stimulate the production of collagen by fibroblasts. In this phase, new blood vessels are formed and the extracellular matrix is formed intensively.
The final, reconstructive, healing phase after fractional laser exposure lasts several months.
On the 5th day after injury, the "fibronectin matrix" fits along the axis along which the fibroblasts are lined up and along which collagen will be built. An important role in the formation of this matrix is played by transforming growth factor ß (TGF-ß is a strength toxin agent for fibroblasts) as well as other growth factors. The most important form of collagen in the early stages of wound healing is type III collagen (this type of collagen is located in the upper layer of the dermis, just below the basal layer of the epidermis). The longer the phase of change, the more type III collagen is produced, but in any case its amount increases to the maximum from 5 to 7 days after the injury. Collagen type III is gradually replaced by collagen over approx. a yearType I that strengthens the strength of the skin. Blood circulation is gradually normalized, the skin becomes smoother and acquires a natural color.
Comparative analysis of laser methods for skin remodeling
Summarizing above, here is a diagram showing the relationship between the effectiveness and safety of laser skin transformation techniques.
Advantages of Fractional Track Rejuvenation Methods. The benefits of fractional methods used in clinical practice include:
- controlled minimal skin damage. Histological examinations performed after the procedure show an increase in the number of papillae in the dermis, which characterizes the changes in the skin as productive regeneration;
- its effective rejuvenation: the skin becomes thicker, it significantly increases (more than 400% (! )) the production of collagen and elastin;
- short healing time: on average 3 days after FF and 7-14 days after PA;
- minimal risk of hyperpigmentation;
- the ability to perform the procedure in patients with thin skin;
- the ability to have a healing effect on any part of the body;
- the possibility of using light anesthesia types: in fractional photothermolysis, only local anesthesia is used; for fractional abulation, a combination of conduction and infiltration anesthesia is required;
- disappearance of telangiectasias (due to the fact that there is a rupture of blood vessels in many places that their recovery is impossible).
Main indications for fractional treatment

Indications for fractional photothermolysis:
- increase in skin density in the early stages of aging. The FF procedure is relatively easy and can be administered without fear. The therapeutic effect can be exerted on the neck, décolleté, arms, abdomen, thighs, mammary glands;
- skin photography;
- hyperpigmentation, melasma;
- hypertrophic scars;
- stretch marks.
Fractional vent indications:
- wrinkles of varying severity - from fine lines to strongly pronounced (in the form of furrows);
- age-related loss of skin elasticity and firmness;
- excess skin in the eyelids, neck, face (as an alternative to plastic surgery);
- uneven skin structure;
- pronounced photography of the skin;
- acne-ar;
- cicatricial deformity of the skin after injuries, surgeries;
- hyperpigmentation: melasma, lentiginosis, spotted pigmentation, etc.
- vascular dyschromia;
- skin stretch marks;
- actinic keratosis.
Finally, a few words about the prospects for the use of laser technologies in aesthetic medicine. We have to pay tribute to the manufacturers for starting to pay more attention to the safety of medical procedures using lasers. Technology constant evolved. However, the safety of the method was often sacrificed to increase its effectiveness. Or the other way around. A compromise was found in a new principle of delivering laser radiation to tissues. It should be noted that type lasers remained the same: erbium, carbon dioxide, neodymium. This suggests that:
- First, laser skin transformation is recognized as the most effective today;
- secondly, the breadth of coverage of aesthetic and dermatological problems solved by these methods is extremely large - from skin rejuvenation to the treatment of congenital and acquired skin pathologies;
- Third, with the advent of fractional technologies, the safety and effectiveness of treatment have become predictable.